Ear, ear
Dr Sotirios Foutsizoglou provides an introduction to auricular reconstruction
The ear is morphologically unique. The skin of the lateral surface is densely adherent to the perichondrium and is devoid of subcutaneous tissue. The fascial layer between the skin and perichondrium contains a subdermal plexus of vessels. The medial surface of the ear has loosely attached skin containing subcutaneous fat. As a result, skin is relatively more abundant on the medial surface compared with the lateral surface of the ear and has greater mobility. Medial auricular skin provides an excellent donor site for grafts and laps. The skeletal component of the ear consists of elastic cartilage. The unique property of this cartilage, that it is flexible and yet able to maintain a complex topographic contour, distinguishes it from the more rigid cartilage of the nasal septum or rib. Consequently, reconstruction of the ear with rib or septal cartilage results in loss of flexibility of the reconstructed auricle.
The cartilaginous framework is composed of several distinct three-dimensional components. Medially, these components are the conchal, antihelical, antitragal, helical, and lobular complexes. These units are critical in planning the reconstruction of defects involving cartilage replacement.
BLOOD SUPPLY
The arterial supply to the auricle is derived from branches of the superficial temporal artery and the postauricular artery. Both vessels arise from the external carotid artery. The medial surface of the ear is supplied by the postauricular artery. The lateral surface is supplied by both the postauricular and superficial temporal arteries, creating two arterial networks. The triangular foss-scapha network is supplied by the helical branch of the superficial temporal artery. The conchal network is supplied by the postauricular artery, which provides septal perforators to the conchal floor. Flap planning and design should give due consideration to these arterial networks. Venous drainage is through the postauricular vein, which drains into the external jugular system. There is supplemental venous drainage from the superficial temporal and retromandibular veins. Lymphatic drainage of the auricle is primarily to the preauricular, infra-auricular, and mastoid lymph nodes.
INNERVATION
The auricle is innervated by contributions from both cranial and spinal nerves. They include the great auricular nerve (C2, C3), the auriculotemporal nerve (V3), the lesser occipital nerve (C2, C3), and a branch of the vagus nerve (X, Arnold’s nerve). The great auricular nerve divides into anterior and posterior branches. The anterior branch supplies the lower half of the lateral aspect of the auricle, while the posterior branch supplies a similar area on the medial surface of the auricle. The auriculotemporal nerve supplies the superolateral surface of the auricle. The lesser occipital nerve supplies the superior aspect of the ear on the medial side. The concha is supplied by Arnold’s nerve.
EMBRYOLOGY
The auricle arises embryologically from the first and second branchial arches. During the sixth week in utero, the external ear begins to develop around the dorsal end of the first branchial cleft. The ear arises from six buds of mesenchyme in the first and second branchial arches, known as the ‘six hillocks of His’.
The anterior hillock gives rise to the tragus, the root of the helix, and the superior helix; the posterior hillock becomes the antihelix, tragus, and lobule. The first branchial groove forms the external auditory meatus and concha. The lobule is the last component of the external ear to form.
Analysis of the dimensions and proportions of the external ear is important for planning reconstructive procedures
EAR ARCHITECTURE
Analysis of the dimensions and proportions of the external ear is important for planning reconstructive procedures. The vertical height of the ear roughly matches the distance between the lateral orbital rim and the root of the helix, at the level of the eyebrow. Ear width is approximately 55% of its length, and the helical rim protrudes between 1cm and 2.5cm from the skull. The angle of protrusion from the skull typically ranges from 25° to 30°. The vertical axis of the ear is inclined posteriorly at an angle of approximately 15° to 20°. The original anatomical descriptions of auricular orientation suggested that the long axis of the ear was roughly parallel to the dorsum of the nose, but it is now widely recognised that the ear is rotated 10° anterior to that plane. The superior level of the ear matches the level of the lateral eyebrow. To account for individual variations in topographic features, positioning, and symmetry, the contralateral ear is used as a template in planning reconstruction, rather than strict adherence to textbook-defined norms. The most important principle of auricular reconstruction is that size, location, and orientation of the reconstructed ear be similar to the normal ear. The dominant features that make an ear recognisable are the helix, tragus, antitragus, and conchal bowl.
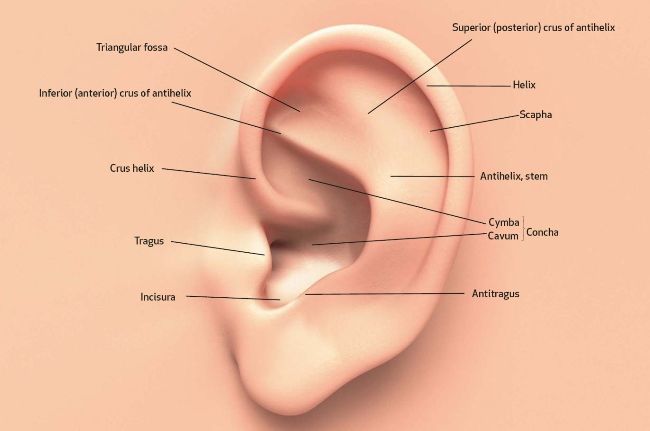
Figure 1: Topographic landmarks of the auricle
GENERAL PRINCIPLES OF SMALL EAR DEFECTS
Auricular defects may be divided into defects of cutaneous coverage, with or without intact cartilage, and defects that are full thickness. Small cutaneous defects of the helical rim may be reconstructed with primary wound closure and occasionally require small excisions of cartilage to avoid distortion. Defects of the densely adherent lateral auricular skin can rarely be closed primarily, whereas those of the more pliable medial surface can often be repaired primarily. The pliability of medial auricular skin permits the harvest of relatively large postauricular skin grafts with primary closure of the donor site. Lateral cutaneous defects that have intact cartilage are best treated with skin grafts, provided there is intact perichondrium over the exposed cartilage. The contralateral postauricular skin is an excellent donor site for a full-thickness skin graft used to resurface the lateral ear. Preauricular skin may also be used with minimal donor site morbidity. In cases in which the perichondrium is absent, resulting in an avascular surface, cartilage may be removed if it is not critical to auricular shape. Windows created through the cartilage provide surface contact between the graft and the vascularised subcutaneous tissue of the medial aspect of the auricle. The cartilage of the concha, fossa triangularis, and scapha are amenable to partial removal without loss of the structural integrity of the ear. The cartilaginous windows provide access to the perichondrium of the medial aspect of the ear, which in turn provides suicient vascularity for successful skin grafting.
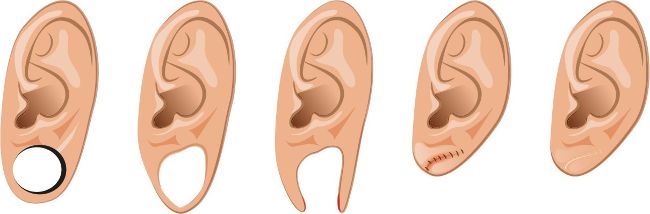
Figure 2. Earlobe repair
Surgical approaches for the reconstruction of defects of the skin and underlying cartilage include converting the defect into a full-thickness, wedge-shaped excision, followed by primary wound closure, and employing a composite graft or lap that incorporates structural support. The size and location of the defect dictate which alternative is most appropriate. Defects less than 1.5cm of the helix or antihelix are best repaired by conversion to a wedge-shaped excision. The wound is then repaired primarily and results in a minimally visible scar. Whereas this approach does reduce vertical height of the ear, the difference with the contralateral ear is usually not conspicuous.
When a wedge-shaped excision of the auricle is performed, excessive wound closure tension is avoided by removing a portion of the concha to accommodate advancement of the two borders of the ear defect. If this is not performed, cupping and distortion of the ear will occur. Medium-sized helical defects, from 1.5cm-2cm, can be managed by composite grating from the contralateral ear. Typically, a composite graft half the size of the defect is transplanted from the opposite ear, thereby creating two ears of equal size. The cartilage edges of the graft and the recipient site are securely approximated with a row of interrupted sutures. Graft immobilisation is essential for proper healing and can be accomplished by use of bolster sutures to secure a splint over the ear. De-epithelialisation of the medial aspect of the composite graft and its implantation into a subcutaneous recipient site have been described. The graft if released from the soft tissue attachment in a second surgical stage, an approach that is designed to increase graft survival. Transfer of a composite graft from the contralateral ear exposes both ears to some risk of infection and deformity, so its use must be carefully considered in view of this risk.

SURGICAL RECONSTRUCTION OF THE EARLOBE
Reconstruction of defects of the inferior third of the auricle is generally less dffiicult than repair of defects elsewhere on the ear because of the relative pliability and laxity of auricular and periauricular skin in this region. Up to 50% of the earlobe may be removed by a wedge-shaped excision followed by primary wound closure, yielding only minimal deformity. Total earlobe reconstruction is performed by employing a composite lap containing conchal cartilage in a two-staged procedure.
First, a segment of cartilage, the shape of the earlobe obtained from the contralateral concha, is embedded in a subcutaneous pocket below the auricle in a location corresponding to the desired position of the earlobe. Six weeks later, the cartilage and overlying skin are elevated as a composite lap, based superiorly on the auricle. The medial surface of the composite lap is skin grated and the donor site of the composite lap is closed primarily by advancing the adjacent skin. This technique provides an excellent skin colour match between the lap and the ear, results in minimal local distortion of tissues, produces a naturally shaped and contoured earlobe, and allows precise earlobe positioning.
Earlobe repair is a simple procedure that can be performed in-office. Many patients want to repair the tear or slit caused by years of wearing heavy or dangling earrings or have their enlarged earlobes reduced in size. Many techniques have been described by various surgeons. One simple technique for for dilated ear lobules after gauge ear piercing is shown in figure 2. Another technique is double opposing perpendicular linear repair. This procedure can be performed using local anaesthetic and with 5-0 nylon sutures. The procedure is initiated by scoring a circle within the circular rim of the defect. The scored circle is then undermined to fat. A linear closure is then placed on the anterior aspect of the circular lobular defect, followed by a linear closure on the posterior aspect oriented 90° to that on the anterior surface. A single linear reapproximation of tissue anteriorly and posteriorly in the same direction would distort the lobule and also result in a dogear deformity. Performing a posterior closure perpendicular to the anterior closure corrects the medial and lateral dog-ear deformity resulting from the anterior approximation. Two perpendicularly opposed linear closures pull the ear lobule together in a way such that it is rounded, free of notching, appears natural, and is aesthetically pleasing with minimal scarring.
The importance of earlobe aesthetics can be appreciated following facelift surgery
NON-SURGICAL REJUVENATION OF THE EARLOBE
The lobule is the last component of the external ear to form. It is a fibroadipose structure devoid of cartilage with a length of 1.5-2cm constituting 25-30% of the long axis of the ear.
Age-related earlobe changes include volume loss, elongation, a more concave surface, wrinkly skin, and pigment changes similar to the rest of the facial skin. The importance of earlobe aesthetics can be appreciated following facelift surgery whereby ‘pixie ear’ deformities can be one of the most prominent stigmata of a surgical facelift.
Earlobe delation, concave appearance and rhytids can be easily addressed with HA fillers or collagen stimulating agents using a sandwich technique. I like using a more viscous product to inject deep into the main body of the earlobe to covert the developing age-related concavity into a slight convexity and a less viscous product intradermally using a multipuncture technique in order to ill the supericial rhytids and induce collagen and elastin stimulation.
SUMMARY
When auricular reconstruction is approached systematically, successful results may be achieved. The morphological uniqueness of the auricle, consisting of medial and lateral cutaneous cover over a thin, flexible, and highly convoluted cartilage, causes auricular reconstruction to be a challenge. Constituent components of the defect must be carefully analysed and a plan conceived for the reconstruction of each component. Depending on the size, depth, and anatomical location of the defect, different repair techniques are employed. These range from primary wound closure to skin grating, or the use of local laps and autogenous rib framework grafts. The ultimate goal is a functioning appendage that closely approximates the position, size, and contour of its normal contralateral counterpart. AM


Dr Sotirios Foutsizoglou developed a particular interest in anatomy during his time working in plastic and reconstructive surgery in the NHS. He became heavily involved in teaching anatomy and physiology to medical students and junior doctors and has worked as an anatomy demonstrator for Imperial College. He is currently completing his last year of training in plastic and reconstructive surgery at Evangelismos General Hospital of Athens. Since 2012, in his role as the lead trainer of KT Medical Aesthetics Group, he has been training practitioners in facial anatomy and advanced non-surgical treatments and procedures. He has written and lectured on facial anatomy and complications associated with injectables both nationally and internationally.